Provider and clinic-level correlates of deferring antiretroviral therapy for people who inject drugs: a survey of North American HIV providers
Journal of the Internatinal AIDS Society 2012;15:10
Background. Injection drug users (IDUs) face numerous obstacles to receiving optimal HIV care, and have been shown to underutilize antiretroviral therapy (ART). We sought to estimate the degree to which providers of HIV care defer initiation of ART because of injection drug use and to identify clinic and provider-level factors associated with resistance to prescribing ART to IDUs.
Methods. We administered an Internet-based survey to 662 regular prescribers of ART in the United States and Canada. Questionnaire items assessed characteristics of providers' personal demographics and training, site of clinical practice and attitudes about drug use. Respondents then rated whether they would likely prescribe or defer ART for hypothetical patients in a series of scenarios involving varying levels of drug use and HIV disease stage.
Results. Survey responses were received from 43% of providers invited by email and direct mail, and 8.5% of providers invited by direct mail only. Overall, 24.2% of providers reported that they would defer ART for an HIV-infected patient with a CD4+ cell count of 200 cells/mm3 if the patient actively injected drugs, and 52.4% would defer ART if the patient injected daily. Physicians were more likely than non-physician providers to defer ART if a patient injected drugs (adjusted odds ratio 2.6, 95% CI 1.4-4.9). Other predictors of deferring ART for active IDUs were having fewer years of experience in HIV care, regularly caring for fewer than 20 HIV-infected patients, and working at a clinic serving a population with low prevalence of injection drug use. Likelihood of deferring ART was directly proportional to both CD4+ cell count and increased frequency of injecting.
Conclusions. Many providers of HIV care defer initiation of antiretroviral therapy for patients who inject drugs, even in the setting of advanced immunologic suppression. Providers with more experience of treating HIV, those in high injection drug use prevalence areas and non-physician providers may be more willing to prescribe ART despite on-going injection drug use. Because of limitations, including low response rate and use of a convenience sample, these findings may not be generalizable to all HIV care providers in North America.
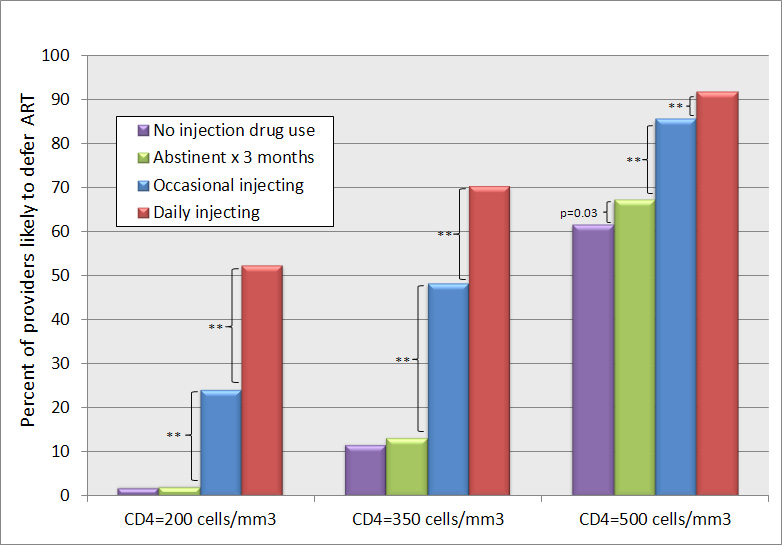
Figure 1. Percentage of providers who would defer ART at three CD4+ levels (200, 350 and 500 cells/mm3) and in four different drug use scenarios (no injecting history, former injecting but abstinent for three months, active but less than daily injecting, and daily injecting).